Hair Thinning vs Hair Loss
Often incorrectly used interchangeably with hair thinning, hair loss and hair thinning are two distinct processes. Hair loss involves the loss of hair from the root and may be a consequence of hair thinning. Hair thinning, in turn involves the conversion of mature hairs called terminal hairs to immature hairs called vellus hairs in a process called follicle miniaturization.
Hair Thinning and Female Pattern Hair Loss
The hallmark feature of Female Pattern Hair Loss is the conversion of large thick hair follicles called terminal hair follicles to short and thin hair follicles called vellus hairs.
Vellus hairs are smaller in length and diameter than terminal hairs. They also are more fragile, prone to easy breaking. An example of vellus hair is the peach fuzz on your earlobe.
The primary cause of Female Pattern Hair Loss is a decrease in the duration of the growth phase (anagen phase) for hair follicles in a characteristic pattern. A shorter period to grow amounts to production of finer hairs with shorter shafts in those regions.
Female Pattern Hair Loss
Female Pattern Hair Loss (FPHL) is the most common form of alopecia in women. Principal to FPHL is follicular miniaturization. The process occurs via both androgen-dependent and androgen-independent mechanisms. Early diagnosis is pivotal as current approved therapy is more effective for preventing progression not reversing loss.
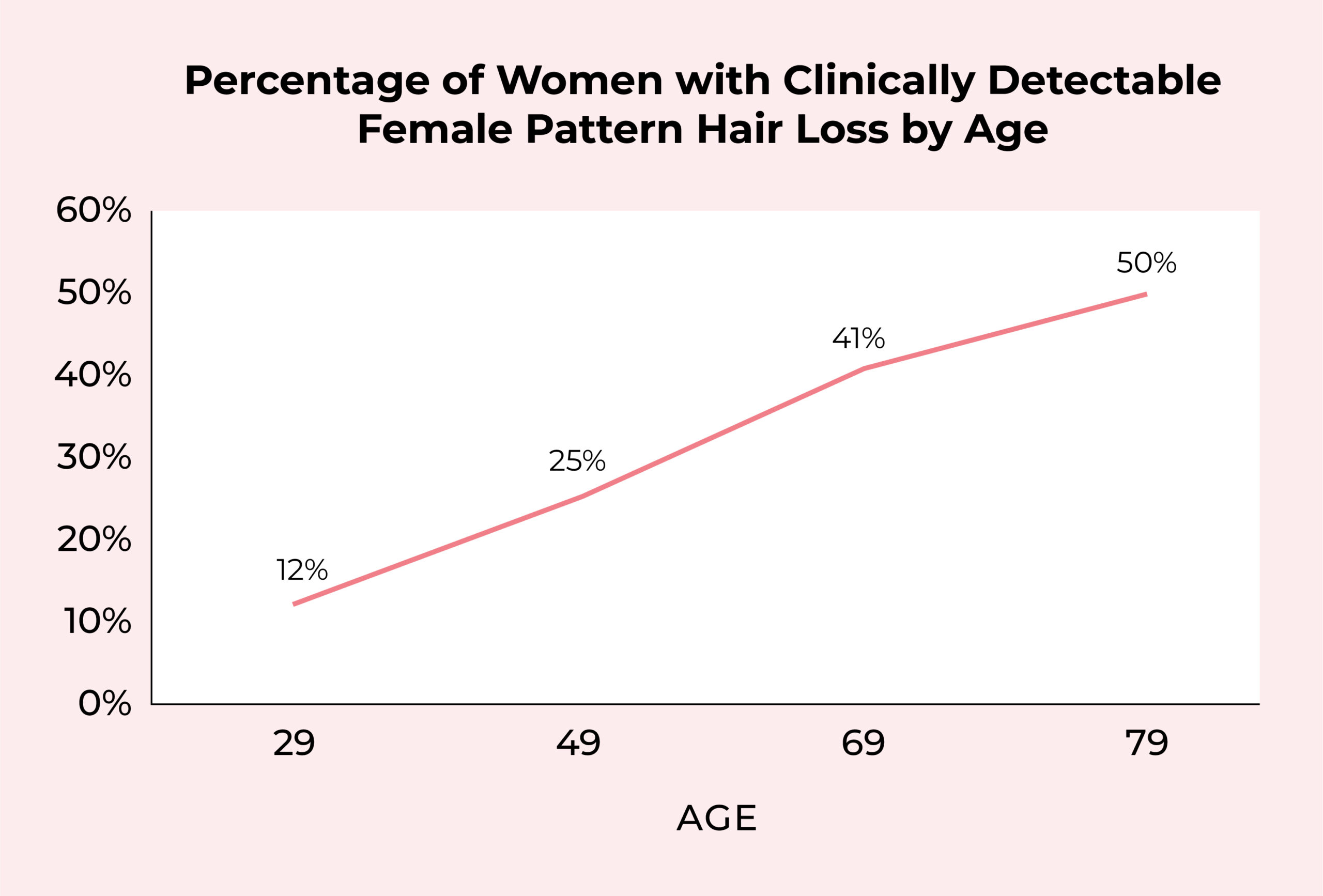
Initial symptoms may develop during teenage years and lead to progressive hair loss following a characteristic pattern. Hair follicles begin miniaturizing and eventually decrease in number primarily in the center, front and parietal scalp regions. By age 49, 25% of women have clinically detectable FPHL, by age 79 more than half of women have some elements of FPHL.
How Do I Know If I Have FPHL?
Diagnosis can be made by a family practitioner. Often a history and exam are sufficient to reach the diagnosis. A biopsy is diagnostic but often unnecessary. The pull test is an evaluation of the number of hairs that are shed after a slight traction on the scalp hair. If more than 10% of hairs grasped are pulled away the pull test is positive and indicative of active shedding. The Pull Test is often unnecessary to make a diagnosis of FPHL as history and characteristic pattern of hair loss are sufficiently diagnostic.
Is There Treatment For Thinning Hair?
First and foremost, it is important to evaluate the need to treat any concurrent diagnosis leading to the thinning. One of the hallmarks of non-scarring alopecias, such as FPHL, is that they maintain their ability to regrow. However, treatment should be weighed against the risks. Many of the treatments affect androgen systems, which is contraindicated during pregnancy. Many practitioners prescribe birth control concomitant to therapy for this reason.
Known treatments focus on slowing progression as opposed to reversing loss. They come in two main categories: systemic and topical.
| Treatment | Mechanism | Comments |
| Minoxidil | Stimulates hair growth by increasing anagen phase. Also promotes blood vessel formation. | Discontinuation may lead to telogen effluvium (excess loss of hair due to stress) |
| Prostaglandin Analog Treatments | Prolongs anagen phase. | Studies in postmenopausal patients failed to demonstrate efficacy. |
| Ketoconazole | Anti-inflammatory, anti-microbial and androgen receptor mediated effects | May potentially have a role whether seborrhea present or not. |
| Melatonin | Increase in anagen to telogen ratio | |
| Platelet-Rich Plasma | Growth factor mediated | Efficacy dependent on quality of PRP |
| Microneedling | Growth factor production and blood vessel formation | Works great in combination with PRP. |
| Light Treatments | Unclear mechanism | Long-term implications of scarring not understood |
| Finasteride (systemic) | 5 alpha reductase inhibitors | Not FDA-approved in women and contraindicated in pregnancy and during lactation. Questionable efficacy in women. |
| Spironolactone (systemic) | Anti-androgen activity. | Off label use. Should be followed by a physician. Potential dose limiting side effects. |
| Oral Minoxidil (systemic) | Same mechanism as topical | Limited by blood pressure effects, fluid retention and indiscriminate growth of hair. |
Hair Transplantation In Women
For women over the age of 25 who have failed medical therapy hair transplantation is a permanent option. Hair transplantation involves the removal of hair follicles from the back and side of the head (the donor region) and carefully placing them in the balding areas (the recipient area).
Modern day hair transplantation comes in two forms. Follicular Unit Transplantation (FUT) is better known as the strip procedure. It involves taking a strip of hair follicles from the donor region to dissect and utilize in bald regions. The area is subsequently sutured closed. The benefit is the ease of obtaining the follicles. The downfall is patient experience, recovery and the scarring that ensues.
Follicular Unit Extraction, or the FUE procedure, involves taking each follicle from the donor region individually. This procedure is the desired procedure as it allows recovery times to decrease drastically and removes the concern for future scarring. The downfall is it requires significant technical skill. As such, many clinics will need to split up procedures over two days in order to achieve desired results. As the field expands more and more clinics will be able to perform the necessary 3000-4000 grafts per session in a day for optimal results.
What Should I Look For In A Hair Transplant Clinic?
Of particular importance to women is preservation of the donor region post-transplant. As the customer base for hair transplantation has been traditionally male dominant, preservation of the donor region was only regarded for its need in future procedures. In women, the stylistic components of the donor region are more frequently leveraged. As such, practitioners will need to focus on optimizing transection rates to best preserve the patient’s donor region.
Design work is crucial for hair transplantation in women. As the majority of practitioners have had a male dominant patient base, many will lack the needed nuance of female hair line design. It is pivotal you find a practitioner who works with you to incorporate your suggestions but guide you in regard to best practices to achieve the desired results. Centrally, hair density becomes equally as important. Your provider should have a strategy for this going in which they should create in discussions with you.
Preferably, the clinic of choice offers no-shave options. During no shave options only a portion of the head is shaved, thereby allowing patients to return to daily living almost immediately.
In Conclusion
Hair thinning involves the creation of shorter, thinner caliber hairs as a manifestation of a shorter hair growth cycle. This is the primary mechanism by which FPHL progresses. By age 80 more than half of women have some sign of FPHL. Treatments do exist but should be weighed against potential risks. Hair transplantation is an underutilized resource for women. When choosing a hair transplant provider, patients should do diligence on their ability to achieve the desired design while preserving the donor area. Clinics that offer no shave procedures are ideal.
Sources
- Bhat Y et al. Female Pattern Hair Loss- An Update. Indian Dermatol Online Journal. 2020. 11(4): 493-501.
- Messenger AG et al. Follicular Miniaturization in Female Pattern Hair Loss: Clinicopathological Correlations. 2006. 155(5):926-930.
- Fabbrocini G et al. Female Pattern Hair Loss: A Clinical, Pathophysiologic and Therapeutic Review. Int J Womens Dermatol. 2018 4(4):203-211.
- Unger R. Female Hair Restoration. Facial Plast Surg Clini North Am 2013. 21(3): 407-17.